 Inflammatory bowel disease (IBD) is a chronic condition affecting the digestive system.
Inflammatory bowel disease (IBD) is a chronic condition affecting the digestive system.
Conventional treatments for IBD often include anti-inflammatory drugs and immunosuppressants. However, more and more studies are looking into the use of probiotics as a potential therapeutic complement for IBD patients.
What is IBD?
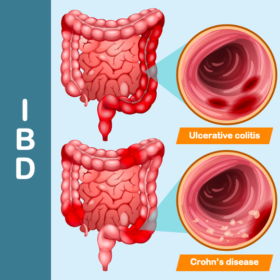
IBD includes Crohn’s disease and ulcerative colitis. Both conditions are characterised by inflammation of the lining of part of the digestive tract, caused by a malfunction of the intestinal immune system.
Crohn’s disease and ulcerative colitis differ in the location of the inflammation. In Crohn’s disease, it can affect the entire digestive tract, whereas in ulcerative colitis, only the rectum and colon are affected.
These diseases alternate between two phases: symptom-free remission phases and active phases during which patients suffer from diarrhoea, abdominal pain, bloody stools, weight loss, fever, fatigue, etc. because of increased inflammation.
These multifactorial pathologies depend on a strong genetic predisposition, a disturbance in mucosal immunity and the epithelial barrier, and dysbiosis.
Can probiotics help?
Probiotics help to rebalance the intestinal microbiota, improving its microbial diversity while limiting the implantation and spread of pathogenic microorganisms.
The role of probiotics in ulcerative colitis has been the subject of several clinical trials. They improve remission induction, with no difference between probiotics and an anti-inflammatory drug used in IBD.
In addition, almost 60% of patients with ulcerative colitis who undergo an ileal-anal pouch anastomosis suffer from pouchitis. This is a non-specific inflammatory process that develops within the ileal reservoir.
The use of probiotics after ileal pouch anastomosis reduced the incidence of pouchitis. They were also effective in maintaining remission and preventing relapse.
In addition, their consumption had an effect on the inflammatory state of the patients:
- By reducing pro-inflammatory cytokines;
- By increasing Treg immune cells;
- By reducing intestinal permeability and modulating the microbiota.
In Crohn’s disease, the dysbiosis of the intestinal microbiota is more marked than in ulcerative rectocolitis, with a reduction in butyrate-producing bacterial species (a short-chain fatty acid) such as Faecalibacterium, Methanobrevibacter and Christensenellaceae. This bacterial imbalance is also thought to depend on the microbial composition at the site of inflammation.
As well as rebalancing the dysbiosis observed in Crohn’s disease, probiotics will help to reduce the recurrence of the disease.
Probiotics appear to offer advantages in the treatment of chronic inflammatory bowel disease. Research into their role in IBD is still ongoing, and further studies are needed to better understand their efficacy and mechanism of action.
LC
References
Picture: Freepik